Confronting the Threat to Biomedical Research
The NIH’s abrupt decision to cap indirect costs at 15% threatens the future of scientific discovery. This policy endangers research institutions, slows progress and weakens U.S. leadership in life sciences. We stand united in opposition and are actively working to reverse this harmful decision.
Our Impact
At Sanford Burnham Prebys, we bring together visionary scientists, emerging technologies and world-class resources.
In a time of dramatic change in biomedical research, our mission remains steadfast: Turn scientific discovery into a healthier world.


Research Centers
Our four disease-focused research centers target the most pressing health threats: cancer, cardiovascular/muscular, neurologic and metabolic disease. They are supported by three enabling technologies centers for drug discovery, multi-omics and computational biology/artificial intelligence, and enriched by four overarching research themes: aging, immunology/inflammation, stem cells/regenerative medicine and children’s health.

Research Programs
Within the research centers are distinct programs that group together researchers working in key areas of biology to foster collaboration and create a stimulating scientific environment. Programs range from cancer epigenetics to degenerative diseases to aging — and support our work to advance scientific discovery to clinical care quickly and smartly.

Education
The Graduate School of Biomedical Sciences and post-doctoral programs recruit and train future generations of diverse scientists, combining hands-on laboratory experience with close mentorship from world-class researchers, buttressed by extensive networking and support services.
Our Central Mission
Our four disease-focused research centers target the most pressing health threats: cancer, cardiovascular/muscular, neurologic and metabolic disease. They are supported by three enabling technologies centers for drug discovery, multi-omics and computational biology/artificial intelligence, and enriched by four overarching research themes: aging, immunology/inflammation, stem cells/regenerative medicine and children’s health.
Discovery Driven
Within the research centers are distinct programs that group together researchers working in key areas of biology to foster collaboration and create a stimulating scientific environment. Programs range from cancer epigenetics to degenerative diseases to aging — and support our work to advance scientific discovery to clinical care quickly and smartly.
Science Shaped
The Graduate School of Biomedical Sciences and post-doctoral programs recruit and train future generations of diverse scientists, combining hands-on laboratory experience with close mentorship from world-class researchers, buttressed by extensive networking and support services.
Latest News
 Jun 30, 2025
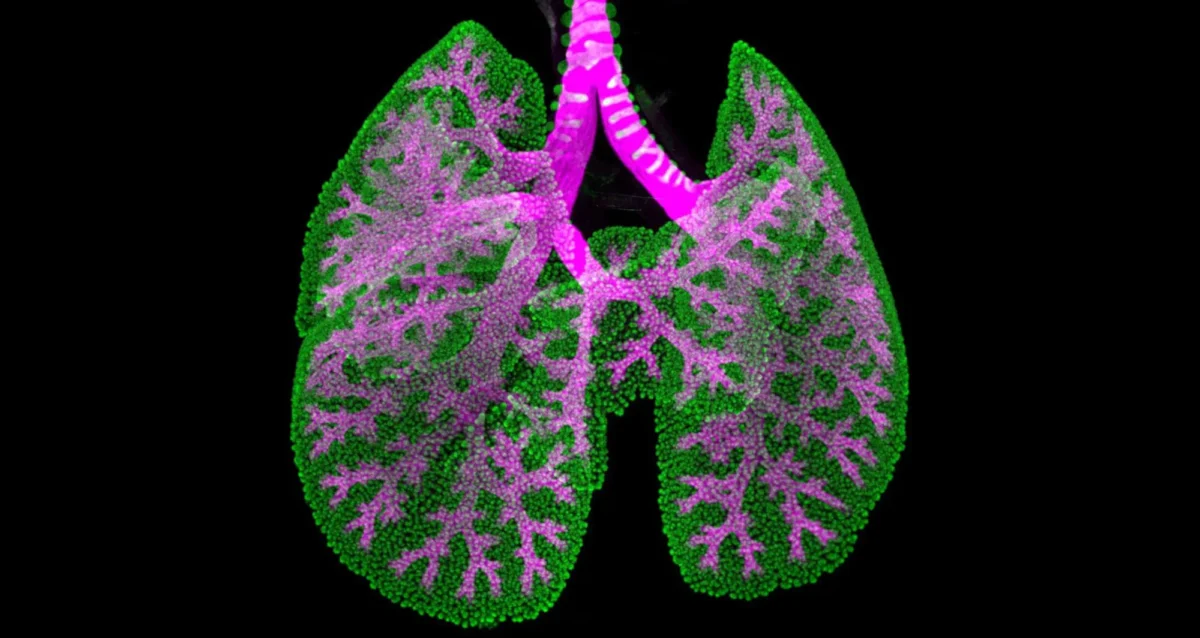
Jun 30, 2025Science in Pictures
Jun 30, 2025A weekly image series featuring selected pictures in science • Lung of an embryonic mouse
 Jun 30, 2025
Jun 30, 2025Leading cancer and metabolic disease expert Michael Karin joins Sanford Burnham Prebys
Jun 30, 2025Karin will direct the Center for Metabolic and Liver Diseases and continue his studies on inflammation and cancer.
 Jun 23, 2025
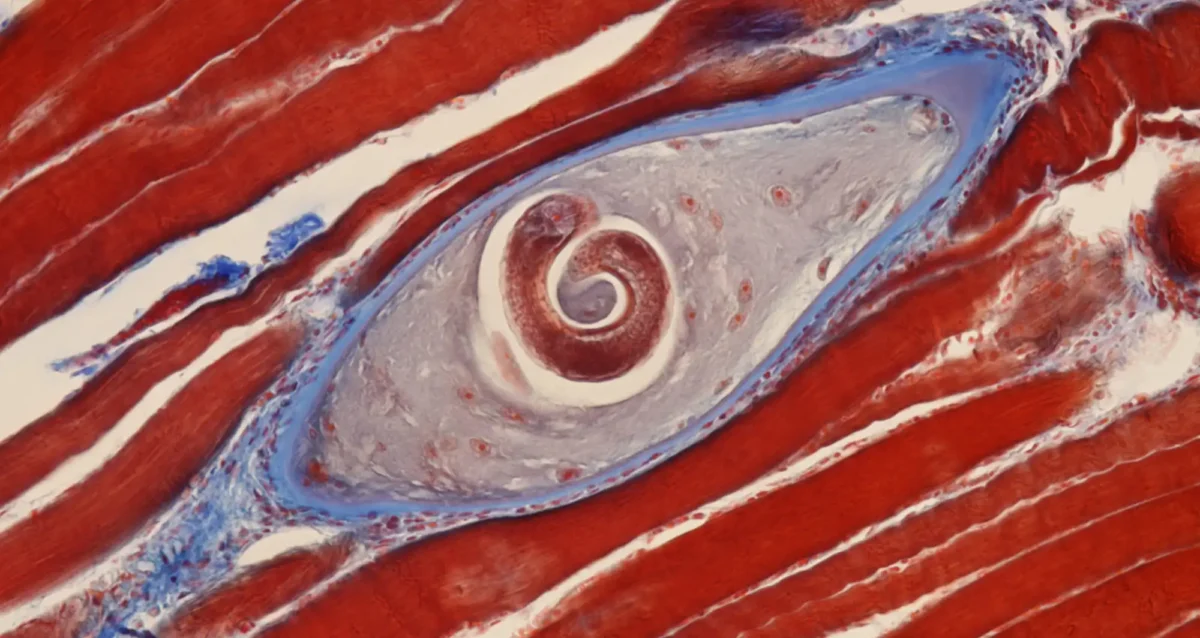
Jun 23, 2025Science in Pictures
Jun 23, 2025A weekly image series featuring selected pictures in science • Trichinella cyst is depicted in pork muscle
 Jun 23, 2025
Jun 23, 2025Opinion: Health database could provide key insights to improve care
Jun 23, 2025Massive amounts of clinical information sit untapped.
 Jun 16, 2025
Jun 16, 2025LEAP scholars share research and celebrate a year of growth
Jun 16, 2025Made possible by the Prebys Foundation, the LEAP (Lab Experience As Pathway) program gives recent college graduates a year of…
 Jun 16, 2025
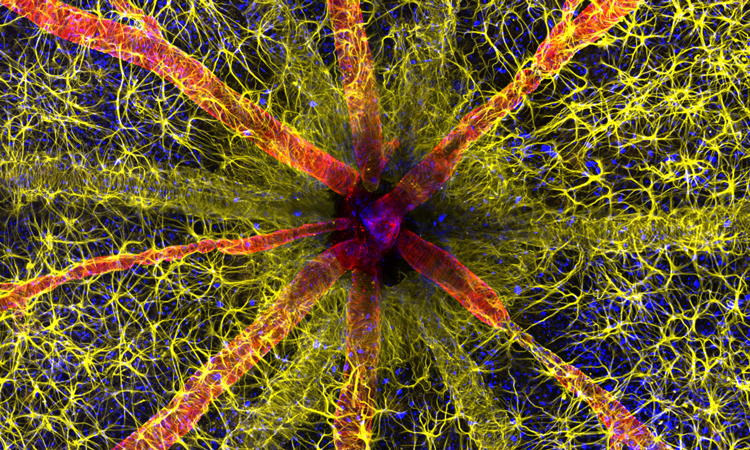
Jun 16, 2025Science in Pictures
Jun 16, 2025A weekly image series featuring selected pictures in science • Optic nerve head of a rodent