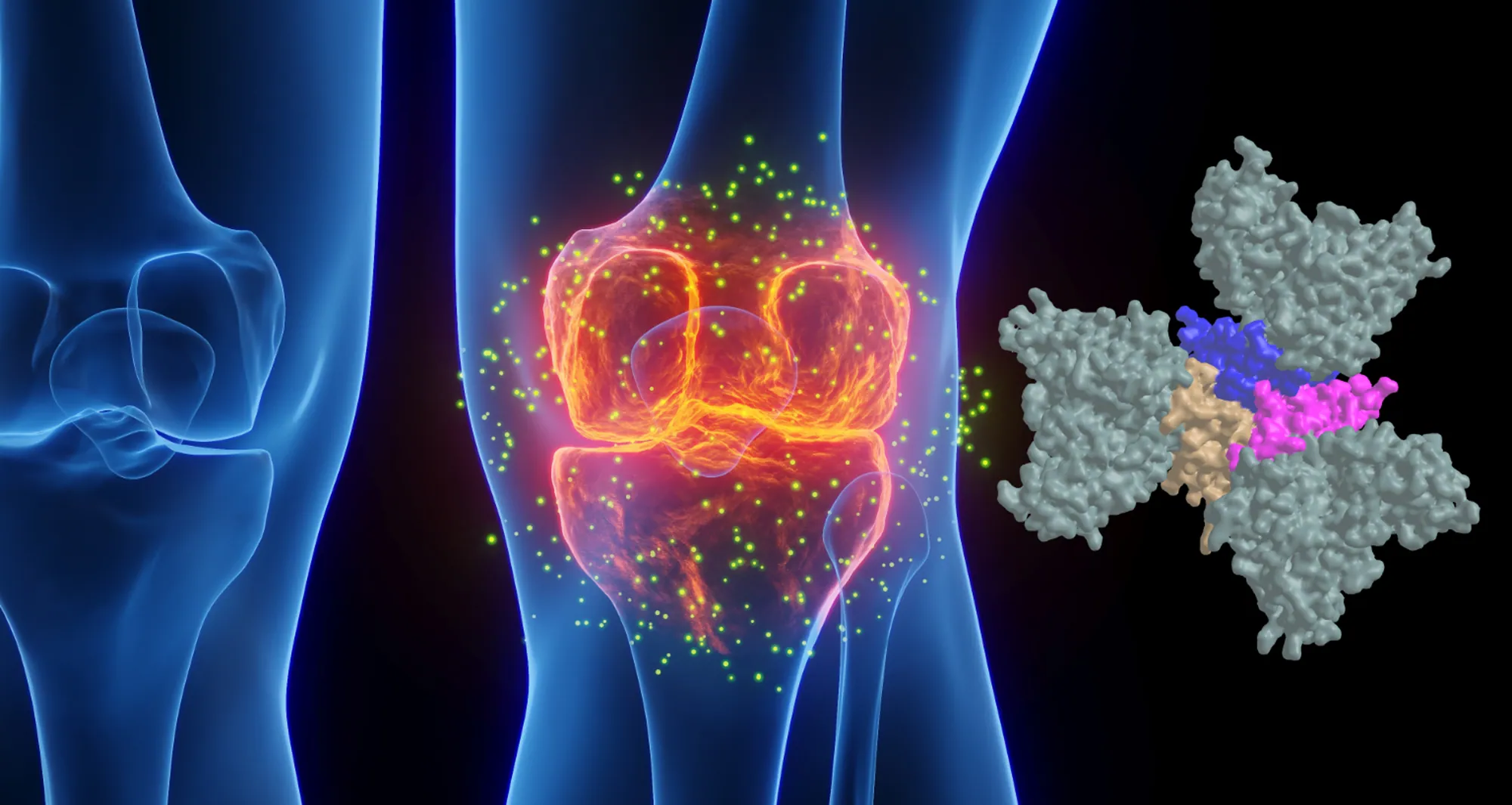
A new study shows that liver cell stress can lead to cancer, yet it also can make tumors less resistant to immunotherapy. The findings may lead to new treatments and help physicians determine which patients will benefit from existing immunotherapies. Image credit: crystal light/Sanford Burnham Prebys.
Cell stress response protein implicated in cancer progression, yet it also weakens resistance to immunotherapies
Metabolic disorders such as obesity and type 2 diabetes place extra stress on the liver. Liver cells try to protect themselves from the accompanying surge in dysfunctional proteins by activating factors that help restore an appropriate protein balance.
One of these factors is a protein called activating transcription factor 6 alpha (ATF6α) that was recently shown to drive the onset of liver cancer if left permanently active. In a Nature study published February 4, 2026, an international team of scientists demonstrated that activating ATF6α in mice caused liver disease that progressed to liver cancer.
In data from human liver cancer patients, ATF6α activation was linked with more aggressive tumors, a suppressed immune system surrounding tumors and reduced patient survival.
The researchers also uncovered ways that ATF6α might be used to advance the treatment of liver cancer. Liver cells with ATF6α switched off developed fewer tumors. While high ATF6α activity levels were associated with cancer progression, they also were found to make tumors more susceptible to certain immunotherapies.
These findings suggest the need for future clinical trials to test drugs that directly target ATF6α to treat the disease. Additionally, it might prove advantageous to screen liver cancer patients for ATF6α activity to find those most likely to benefit from existing immunotherapies.
Randal Kaufman, PhD, is a professor in the Center for Metabolic and Liver Diseases at Sanford Burnham Prebys and a co-corresponding author of the study. Image credit: Sanford Burnham Prebys.
Xin Li, PhD, a postdoctoral fellow at the German Cancer Research Center (DKFZ), shares first authorship of the study with co-corresponding author Cynthia Lebeaupin, PhD, principal scientist at Pfizer and former postdoctoral researcher at Sanford Burnham Prebys Medical Discovery Institute.
The other co-corresponding authors are Dirk Haller, PhD, Technische Universität München; Randal Kaufman, PhD, Sanford Burnham Prebys; and Mathias Heikenwälder, PhD, University of Tübingen and DKFZ.
Institute News
Protein superfamily crucial to the immune system experiences Broadway-style revival
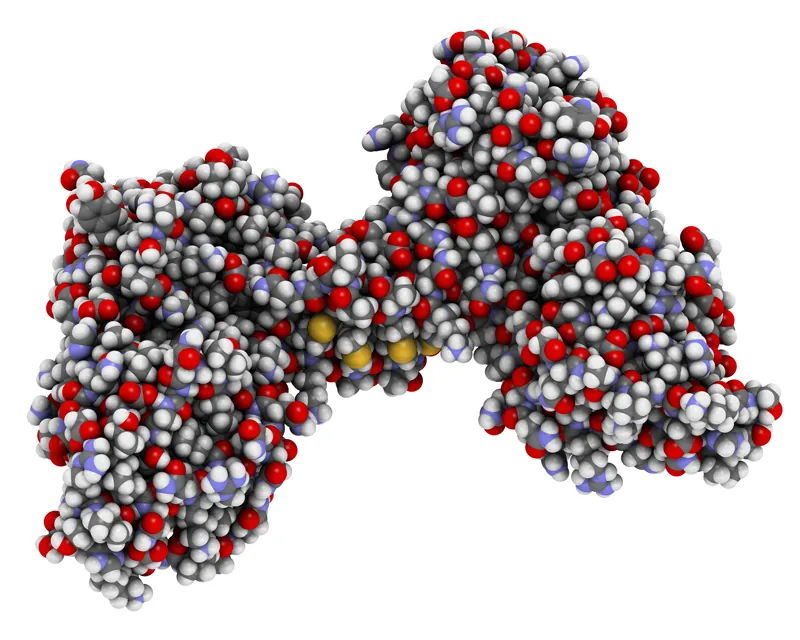
Tumor necrosis factor-α (TNF), shown in pink and tan, is part of a large family of signaling proteins known to play a key role in developing and coordinating the immune system. Here, TNF is depicted in a complex with an antibody called golimumab, pictured in slate gray. Golimumab is used as a drug to treat rheumatoid arthritis and other autoimmune disorders, which it does by smothering the receptors on TNF that initiate inflammation.
More than 25 years after targeting a member of this superfamily of proteins led to groundbreaking treatments for several autoimmune diseases including rheumatoid arthritis and Crohn’s disease, San Diego scientists note a resurgence of interest in research to find related new drug candidates.
In 1998, the same year “Footloose” debuted on Broadway, REMICADE® (infliximab) was approved by the FDA for the treatment of Crohn’s disease. This was the first monoclonal antibody ever used to treat a chronic condition, and it upended the treatment of Crohn’s disease.
Research published in February 2024 demonstrated better outcomes for patients receiving infliximab or similar drugs right after diagnosis rather than in a “step up” fashion after trying other more conservative treatments such as steroids.
Infliximab and ENBREL® (etanercept) — also approved in 1998 to treat rheumatoid arthritis — were the first FDA-approved tumor necrosis factor-α (TNF) inhibitors. TNF is part of a large family of signaling proteins known to play a key role in developing and coordinating the immune system.
The early success of infliximab and etanercept generated excitement among researchers and within the pharmaceutical industry at the possibility of targeting other members of this protein family. They were interested in finding new protein-based (biologics) drugs to alter inflammation that underlies the destructive processes in autoimmune diseases.
As “Footloose” made it back to Broadway in 2024 for the first time since its initial run, therapies targeting the TNF family are in the midst of their own revival. Carl Ware, PhD, a professor in the Immunity and Pathogenesis Program at Sanford Burnham Prebys, and collaborators at the La Jolla Institute for Immunology and biotechnology company Inhibrx, report in Nature Reviews Drug Discovery that there is a resurgence of interest and investment in these potential treatments.
“Many of these signaling proteins or their associated receptors are now under clinical investigation,” said Ware. “This includes testing the ability to target them to treat autoimmune and inflammatory diseases, as well as cancer.”
Today, there are seven FDA-approved biologics that target TNF family members to treat autoimmune and inflammatory diseases. There also are three biologics and two chimeric antigen receptor (CAR)-T cell-based therapies targeting TNF members for the treatment of cancer. This number is poised to grow as Ware and his colleagues report on the progress of research and many clinical trials to test new drugs in this field and repurpose currently approved drugs for additional diseases.
“The anticipation levels are high as we await the results of the clinical trials of these first-, second- and — in some cases — third-generation biologics,” said Ware.
Ware and his coauthors also weighed in on the challenges that exist as scientists and drug companies develop therapies targeting the TNF family of proteins, as well as opportunities presented by improvements in technology, computational analysis and clinical trial design.
Carl Ware, PhD, is a professor in the Immunity and Pathogenesis Program at Sanford Burnham Prebys.
“There are still many hurdles to get over before we truly realize the potential of these drugs,” noted Ware. “This includes the creation of more complex biologics that can engage several different proteins simultaneously, and the identification of patient subpopulations whose disease is more likely to depend on the respective proteins being targeted.
“It will be important for researchers to use computational analysis of genetics, biomarkers and phenotypic traits, as well as animal models that mimic these variables. This approach will likely lead to a better understanding of disease mechanisms for different subtypes of autoimmune conditions, inflammatory diseases, and cancer, enabling us to design better clinical trials where teams can identify the appropriate patients for each drug.”
Institute News
Decades of dedication led to FDA approval of a new treatment for Duchenne Muscular Dystrophy
Lorenzo Puri with his lab in Rome in 2004. From left: Lucia Latella, PhD; Silvia Fortuni, PhD; Christian Reale, PhD; Puri; Giulia Minetti, PhD; Cristiano Simone, PhD; and Carlo Serra, MD.
Nearly 30 years of discoveries by a Sanford Burnham Prebys scientist and collaborators lead to federal approval of the first non-steroidal drug to treat Duchenne muscular dystrophy.
For one San Diegan scientist at Sanford Burnham Prebys, the March 2024 federal approval of a new drug to treat Duchenne muscular dystrophy (DMD) marked a milestone in three decades of studying muscle regeneration and muscle-wasting diseases.
The compound, called Givinostat and marketed as DUVYZAT™, is a histone deacetylase inhibitor (HDACi)and was approved by the FDA for the treatment of boys with DMD.
“I have been working from the very beginning of my research career to translate early, basic discoveries into a treatment for DMD,” said Pier Lorenzo Puri, MD, director and professor in the Development, Aging and Regeneration Program at Sanford Burnham Prebys. “The lack of effective treatments for boys with DMD has left families and patients hopeless since the discovery of this disease. Witnessing the progression of such a disease without any option to counter its progression is cruel and I felt the urgency to help these people.”
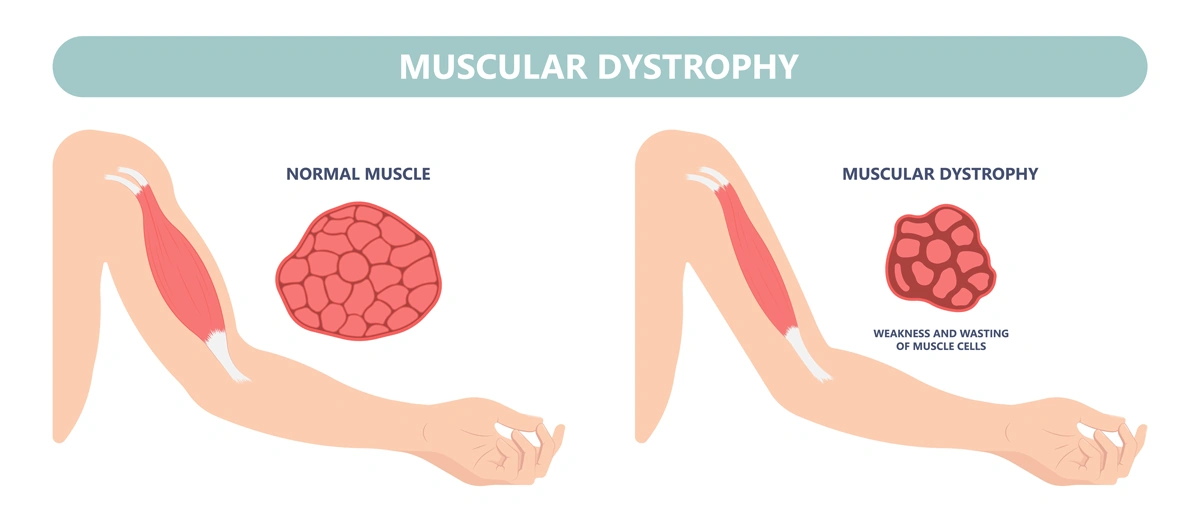
DMD is the most frequent form of muscular dystrophy affecting approximately 1 in 3,500 male births. DMD is linked to the chromosome X, which harbors the gene coding the protein called dystrophin. As such, the disease develops only in males receiving from their mother the X chromosome carrying mutations in the dystrophin gene that impair production of dystrophin. Dystrophin is a protein that protects muscles from degeneration after they contract and relax. In its absence, the muscles of boys with DMD are prone to damage and undergo cycles of contraction and degeneration that eventually lead to muscle wasting and reduced function.
For decades, steroids have provided the standard-of-care for DMD, but steroids represent an empirical and palliative treatment based on their general anti-inflammatory properties, rather than a treatment that targets specific pathological events that contribute to DMD progression. Moreover, the chronic use of steroids is complicated by many side effects, including weight gain, weak bones, high blood pressure and behavior changes.
Puri decided to focus on the potential use of HDACi to treat DMD after he made seminal basic discoveries that revealed how muscle growth and regeneration are regulated by two enzymes with opposing activities: histone acetyltransferases and deacetylases.
“HDACi are not going to cure muscular dystrophy, but they do provide the first pharmacological treatment that can delay DMD progression, regardless of the type of mutation, and do so in a financially affordable way,” said Puri.
The molecular structure of dystrophin, a protein that protects muscles from degeneration after they contract and relax.
“It is important to note that FDA approval of Givinostat is not the end of the journey, but the beginning. The very good news here is that there is room to improve the efficacy of HDACi-based treatment for DMD by using already existing compounds or by developing novel molecules endowed with an improved therapeutic potential. This is because Givinostat has been used at sub-optimal concentrations due to potential adverse effects, and this might have limited its efficacy as a HDACi.
“People ask me whether Givinostat was approved because it is the most effective molecule among existing HDACi. The answer is that Givinostat has been the first, and so far the only, HDACi to be tested in clinical trials for boys with DMD. Givinostat might not entirely express the therapeutic potential of HDACi for DMD. A reasonable and exciting goal of future studies is to identify HDACi that surpass Givinostat in terms of therapeutic efficacy.”
Without dystrophin, the muscles of boys with Duchenne muscular dystrophy are prone to damage and undergo cycles of contraction and degeneration that eventually lead to muscle wasting and reduced function.
Puri noted that, “It is also important to carefully investigate functional interactions between HDACi and steroids, as the clinical trial with Givinostat has been performed while research participants were receiving steroids. However, because the activity of steroids is largely dependent on HDAC, it is very likely that these two treatments could collide, rather than synergize in producing beneficial effects on the muscles of DMD boys.”
He also emphasized that the impact of FDA approval of Givinostat extends way beyond the possibility to offer a treatment for DMD.
“It is the first evidence that it is possible to treat DMD by targeting pathogenic events induced as a consequence of dystrophin deficiency, as an effort parallel to gene and cell therapy, which will hopefully converge into future and more effective combined therapies.”
Building the basic science foundation
Puri’s contributions to the approval of the first non-steroidal drug to treat DMD span nearly 30 years of basic and preclinical research of diseases thought to be incurable — especially pediatric conditions he thought especially cruel.
The puzzle pieces began to take shape as Puri was studying the growth of muscle cells and skeletal muscle tissue, a biological process called skeletal myogenesis. He started working on this project in the 1990s in the laboratory of molecular biology directed by Massimo Levrero, MD, in Rome. Puri had earned his medical degree in 1991 before conducting an internship in Internal Medicine.
“I started there, in a lab inside a hospital in Rome,” said Puri. “I used to see patients until the early afternoon and then I was running to the lab to perform experiments. As a young clinician with a passion for basic research, I was always developing experiments with patients in mind.”
Puri decided to test his first hypothesis by using what was then an innovative technology called microinjection to insert DNA or antibodies inside cultured cells. He decided to spend several months at the Free University of Berlin in the laboratory of Adolf Graessmann, PhD, a pioneer of this technique. Puri later decided to go to the United States to work in the lab of Jean Y.J. Wang, PhD, at the University of California San Diego, to further develop his studies.
After entering the U.S., Puri has worked closely with his long-term collaborator and friend Vittorio Sartorelli, MD, currently the deputy scientific director of the National Institute of Arthritis and Musculoskeletal and Skin Diseases and chief of the institute’s Laboratory of Muscle Stem Cells & Gene Regulation. Together, they uncovered an important role for two groups of enzymes, histone acetyltransferases and deacetylases, that control access to DNA by altering the structure of chromatin.
Histone acetyltransferases control DNA accessibility by adding acetyl groups to histones, which loosens the wrapping of DNA around them, essentially ‘opening’ chromatin and promoting gene expression. Histone deacetylases reverse the process by removing acetyl groups, limiting the activity of genes and the production of key proteins.
“One of our seminal findings was the discovery of associations between myogenesis and an enzymatic activity that could be pharmacologically modulated,” explains Puri.
Puri with current members of hislab at Sanford Burnham Prebys.
Puri and Sartorelli started to explore the possibility that pharmacological modulators of this process by HDACi could affect the growth of muscle cell progenitors and their ability to form contractile muscle tissues.
After finding that HDACs limit muscle cell differentiation, the team’s next step was to find compounds (inhibitors) capable of blocking HDACs from removing acetyl molecules and reducing myogenesis. “We decided see if there is an HDAC inhibitor — an inhibitor of the inhibitor — because this could reduce muscle loss,” notes Puri. “There were a few compounds, and we found a strong effect every time we tested them.”
“I remember vividly the first time I saw the effect of HDACi on cultured muscle cells. I was a postdoc in Jean Wang’s lab at UC San Diego, and one morning I opened the incubator and found that muscle cells treated with HDACi had formed giant myotubes (the contractile muscle). Of course, we started to wonder whether such evidence could provide the rationale we were looking for. If so, this could pave the way toward discovering pharmacological interventions that may promote muscle regeneration.
Puri with Chiara Mozzetta, PhD, faculty at the Institute of Molecular Biology and Pathology at the National Research Council of Italy. Mozzetta previously conducted a postdoctoral fellowship in the Puri lab and made major contributions to the discovery of HDAC inhibitors as therapeutics for DMD.
“But, at that time, it sounded more like a dream. We did not even dare to imagine that the final outcome would have been the identification of a pharmacological treatment for DMD.”
Pursuing the preclinical potential
Puri and Sartorelli pursued their dream, driven by encouraging experimental evidence and discoveries. Still, it took years to provide the rationale for testing HDACi in DMD—years and a few fortunate coincidences. One was the identification of follistatin as a mediator of the action of HDACi on muscle cells. Follistatin is the endogenous inhibitor of myostatin, a potent inhibitor of muscle growth and size, ensuring that muscles do not grow too large.
It was during that time that other groups independently discovered that genetic mutations in the myostatin gene resulted in an abnormal increase in muscle mass in cattle, mice and humans. More importantly, it was published that genetic or pharmacological inactivation of myostatin could exert beneficial effects in a mouse model of DMD.
“That discovery suggested the rationale of testing whether HDACi could exert similar beneficial effect in the same mouse model of DMD,” said Puri. The team hypothesized that this could be achieved by using HDACi to block myostatin activity through the induction of follistatin.
Puri and Sartorelli decided to treat mdx mice — the mouse model of DMD — with a few HDACi. Puri performed these studies with a group of investigators that worked synergistically in his two labs (one in San Diego and the Dulbecco Telethon Institute laboratory in Rome) and in collaboration with Italian scientists Carlo Gaetano, PhD, and Claudia Colussi, PhD.
“The results of the experiment went beyond the most optimistic expectations,” said Puri. “The muscles were bigger. There was no scar tissue, no abnormal fatty deposits and less inflammation. The treated mice were running like normal mice.”
In follow-up studies, Puri and collaborators realized that the therapeutic properties of HDACi extended beyond the targeting of follistatin/myostatin interactions. The pace of discoveries increased along with the improved knowledge on DMD pathogenesis. Key and timely information was gained through identification of a population of muscle interstitial cells, called fibro-adipogenic progenitors (FAPs), from the laboratories of Fabio Rossi, MD, PhD, at the University of British Columbia in Canada and Dr. Kunihiro Tsuchida, MD, PhD, at Fujita Health University in Japan.
FAPs support muscle regeneration of normal muscles, but in dystrophin-deficient muscles these cells turn into the main effectors of fibrotic scars and fat infiltration — the most deleterious events in DMD pathogenesis. Studies from the Puri lab demonstrated that HDACi could restore the ability of FAPs from DMD muscles to promote regeneration, while blocking their pro-fibrotic and adipogenic activity.
Puri with collaborator Vittorio Sartorelli, MD, the deputy scientific director of the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
“The identification of FAPs was a lucky coincidence, as it provided one of the main cell types targeted by HDACi and enabled the identification of the molecular mechanism of action that accounts for the therapeutic properties of HDACi,” said Puri.
Puri (at right) with collaborator Fabio Rossi, MD, PhD, professor of Medical Genetics at the University of British Columbia in Canada, at a muscle research meeting in Montrealin July 2024.
“It also helped to set in our preclinical studies the parameters that have been used in clinical trials. Indeed, I believe that one of the reasons for the success of this journey has been the development of a solid scientific rationale. I was definitely fortunate to have worked with a team of incredibly skilled young scientists that shared with me the wish to help DMD patients and the perseverance to take on a challenge for over 20 years. Overall, discovering the MOA of HDACs has been a fantastic journey.”
“Although the evidence that HDACi could be used to treat DMD was strong and the rationale was very solid, it was hard to convince big pharma to invest on this treatment. There were many excellent HDACi in the market that could have been used, but after knocking on many doors, no one was willing to partner on this task.
Puri felt compelled by these results to keep building support to convince potential industry partners to develop clinical trials. After talking with many businesses, he found Italfarmaco, an Italian pharmaceutical company with an HDAC inhibitor called Givinostat.
“In the end, I had to knock on the door of Italfarmaco, which owned Givinostat — an HDACi that I had never tested in my previous preclincial studies. This was another coincidence since Dr. Christian Steinkulher, a friend and colleague, alerted me about the potential availability of a pan-HDACi called Givinostat from Italfarmaco.
“When I approached Italfarmaco, I immediately realized that they were not very well prepared to take on this type of research. They were not familiar with DMD, and they didn’t have any previous experience on muscular diseases. They also had no background on the epigenetic effects of Givinostat.
“Until that time, they used Givinostat mostly for its anti-inflammatory properties, rather than the epigenetic regulation of gene expression. However, Italfarmaco recognized some potential in this operation and decided to give to me the opportunity to perform preclinical studies with Givinostat for DMD.”
Clinical trials and regulatory approval
After additional preclinical studies to better understand how Givinostat worked, Italfarmaco informed Puri that the company was ready to develop a clinical trial.
The results of the phase II clinical trial were published in Neuromuscular Disorders in 2016. During the trial, the scientists looked at whether the composition of the muscle improved. Muscle biopsies taken from 19 subjects who were treated for more than a year demonstrated that the drug had caused an increase in muscle fiber area and a decrease in fat deposition, scar tissue and other hallmarks of DMD.
“It was remarkable to see that the same positive effects observed in mdx mice treated with HDACi were also observed in DMD boys treated with Givinostat,” noted Puri. “The reproducibility of the outcomes in preclinical studies and clinical trials emphasizes the importance of performing accurate preclinical studies and identifying reliable outcome measures, as we did with HDACi for DMD.”
The trial also helped the team determine what dose of Givinostat was safe and still effective to use in the pivotal phase III trial that was reviewed by the FDA before the agency granted approval.
Italfarmaco established ITF Therapeutics in January 2024 as a new division that is now responsible for marketing DUVYZAT™ in the U.S. ITF Therapeutics announced that the drug was available in the U.S. on July 25. Italfarmaco’s Marketing Authorization Application (MAA) for Givinostat to the European Medicine Agency (EMA) was validated in fall 2023. This means that the drug is eligible to be reviewed by the EMA. If approved, Givinostat can be made available throughout the European Union (EU).
Puri surfs a wave in San Diego. Surfing is his passion outside of the laboratory.
Paving the way forward
Puri is not resting on his laurels and the approval of the first non-steroidal drug to treat DMD.
“Right now, we have steroids, HDAC inhibitors and gene therapy. We are working on the idea that gene therapy and HDAC inhibitors without steroids can perfectly synergize.”
Lorenzo and his dog Mojo.
The researchers are also investigating ways to enhance the effect of HDAC inhibitors through the use of extracellular vesicles (EV) released from FAPs following the exposure to HDACi. EVs are small biological bubbles that the body uses to carry compounds between cells. They are non-immunogenic and therefore suitable for transplantation into dystrophic muscles.
Puri is also investigating whether there are treatment conditions (including dietary supplements or other synergistic molecules) that can improve the therapeutic efficacy of HDACi. The researchers want to test if HDAC inhibitors can treat other forms of muscular dystrophy beyond DMD.
As much as Puri is focused on the future and continuing to find new and better approaches to treat muscular dystrophy, he also appreciates the importance of this vital moment and how the FDA’s decision positions the field for even more innovation.
“While muscular dystrophy was formally described by scientists 40 years ago, it has been a part of the human story since the beginning. People have been chasing something that could help, and for so long there was nothing to offer. Right now, we are paving the way for even better treatments that will be found.”
More information on the development of HDACi as a treatment for DMD is available in the following manuscripts:
Puri P.L., Avantaggiati M.L., Balsano C., San N., Graessmann A., Giordano A., and Levrero M. p300 is required for MyoD-dependant cell cycle arrest and muscle specific gene transcription. EMBO J. 16,369-383 (1997)
Puri P.L., Sartorelli V., Yang X.J., Hamamori Y., Ogrizko , Howard B., Kedes L, Wang J.Y.J., Graessmann A., Nakatani Y., Levrero M. Differential roles of p300 and PCAF acetyltransferases in muscle differentiation. Mol. Cell 1, 35-45 (1997)
Sartorelli V*., Puri P.L.* , Hamamori Y, Ogrizko V., Nakatani Y., Wang J.Y.J., Kedes L. Acetylation of MyoD directed by PCAF is necessary for the execution of the muscle program. Mol. Cell. 4, 725-734 (1999). *equal contribution
Puri P.L., Iezzi, S., Stiegler P., Chen T.T., Shiltz L., Muscat G., Giordano A, Wang J.Y.J. and Sartorelli V. Class I histone deacetylases sequentially interact with MyoD and pRb during skeletal myogenesis. Mol Cell. 8, 885-897 (2001)
Iezzi S., Cossu G., Nervi C. Sartorelli V., and Puri P.L. Stage-specific modulation of skeletal myogenesis by inhibitors of nuclear deacetylases Proc. Natl. Acad. Sci 99, 7757-7762 (2002)
Iezzi S., Di Padova M., Serra C., Caretti G., Simone C., Maklan E., Zhao P., Hoffman E., Puri P.L. and Sartorelli V. Deacetylase Inhibitors Increase Muscle cell Size by Promoting Myoblast Recruitment and Fusion Through Induction of Follistatin. Dev. Cell. 5:673-84. (2004).
Minetti G. C., Colussi c., Adami R., Serra C., Mozzetta C., Parente V., Illi B., Fortuni S., Straino S., Gallinari P., Steinkhuler C., Capogrossi M., Sartorelli V., Bottinelli R., Gaetano C., Puri P.L. Functional and morphological recovery of dystrophic muscles in mice treated with deacetylase inhibitors. Nature Medicine 12 (10): 1147-50 (2006)
Colussi C., Mozzetta C., Gurtner A. , Illi B., Straino S., Ragone G., Pescatori M., Zaccagnini G., Rosati G., Minetti G., Martelli F., Ricci E., Piaggio G., Gallinari P., Steinkulher C., Capogrossi M.C., Puri P.L*, Carlo Gaetano*. A Common Epigenetic Mechanism Underlies Nitric Oxide Donors and Histone Deacetylase Inhibitors Effect in Duchenne Muscular Dystrophy. Proc. Natl. Acad. Sci 105, 19183-7 (2008) *Corresponding authors. PMCID:PMC2614736.
Mozzetta C., Consalvi S., Saccone V., Tierney M., Diamantini A., Mitchel K.J., Marazzi G., Borsellino G., Battistini L., Sassoon D., Sacco A., Puri P.L. Fibroadipogenic progenitors mediate the ability of HDAC inhibitors to promote regeneration in dystrophic muscles of young, but not old mdx mice. EMBO Mol. Med. (2013), Apr;5(4):626-39 doi: 10.1002/emmm.201202096. [Epub ahead of print]. PMC Journal In Process.
Consalvi S, Mozzetta C, Bettica P, Germani M, Fiorentini F, Del Bene F, Rocchetti M, Leoni F, Mascagni P, Puri P.L., Saccone V. Preclinical studies in the mdx mouse model of Duchenne Muscular Dystrophy with the Histone Deacetylase inhibitor Givinostat. Mol Med. 2013 Mar 27. doi: 10.2119/molmed.2013.00011. [Epub ahead of print]. PMCID: PMC3667212.
Saccone V, Consalvi S, Giordani L, Mozzetta C, Barozzi I, Sandoná M, Ryan T, Rojas-Muñoz A, Madaro L, Fasanaro P, Borsellino G, De Bardi M, Frigè G, Termanini A, Sun X, Rossant J, Bruneau BG, Mercola M, Minucci S, Puri P.L. HDAC-regulated myomiRs control BAF60 variant exchange and direct the functional phenotype of fibro-adipogenic progenitors in dystrophic muscles. Genes & Development. 2014 Apr 15;28(8):841-57. doi: 10.1101/gad.234468.113. Epub 2014 Mar 28.
Bettica P, Petrini S, D’Oria V, D’Amico A, Catteruccia M, Pane M, Sivo S, Magri F, Brajkovic S, Messina S, Vita GL, Gatti B, Moggio M, Puri P.L., Rocchetti M, De Nicolao G, Vita G, Comi GP, Bertini E, Mercuri E. Histological effects of givinostat in boys with Duchenne muscular dystrophy.Neuromuscul Disord. 2016 Jul 11. pii: S0960-8966(16)30069-4. doi: 10.1016/j.nmd.2016.07.002. [Epub ahead of print]
Consalvi S, Tucciarone L, Macrì E, De Bardi M, Picozza M, Salvatori I, Renzini A, Valente S, Mai A, Moresi V, Puri P.L.. Determinants of epigenetic resistance to HDAC inhibitors in dystrophic fibro-adipogenic progenitors. EMBO Rep. 2022 Jun 7;23(6):e54721. doi: 10.15252/embr.202254721. Epub 2022 Apr 4. PMID: 35383427
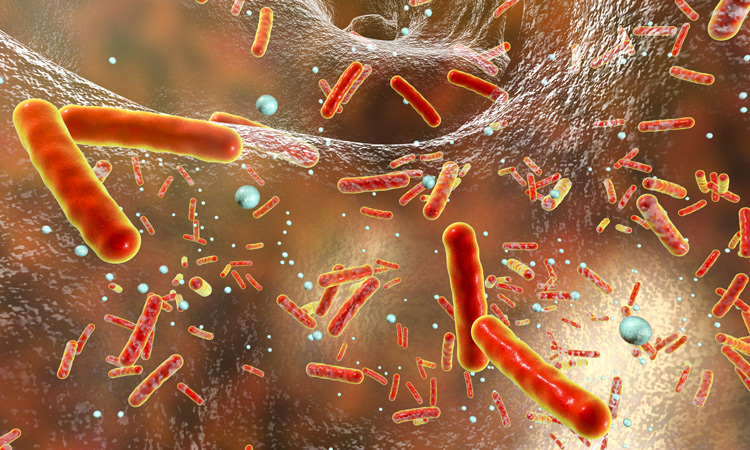
Researchers from Sanford Burnham Prebys have teamed up with prominent drug developer Roche Pharma to learn how bacteria develop antibiotic resistance.
Their new results, published in the journal mBio, are one piece of a long-standing collaboration between the two organizations, the goal of which is to mitigate the growing threat of antibiotic resistance by developing more “irresistible” drugs and by helping improve antibiotic prescribing practices.
“The emergence of antibiotic resistance is inevitable for any single drug, new or old. It’s only a question of time,” says senior author Andrei Osterman, PhD, a professor at Sanford Burnham Prebys. “But the precise time is different for every drug and every microbe, so studying when and how resistance to antibiotics evolves gives us powerful information for improving antibiotic treatment.”
Antibiotic resistance develops rapidly
When a patient is treated with antibiotics, most individual bacteria die, but a few cells will survive, usually as a lucky consequence of a random genetic mutation. These survivors go on to multiply into a whole new population of antibiotic-resistant bacteria.
“The development of antibiotic resistance is a strictly Darwinian process, very similar to evolution in larger organisms,” says Osterman. “The difference is that in bacteria, it happens much more rapidly, which makes antibiotic resistance one of the most pressing challenges facing medicine today.”
Although the speed at which evolution occurs in bacteria makes antibiotic resistance a threat, the researchers were also able to take advantage of this speed to study its development. The team cultured three species of bacteria in a morbidostat, a device that allows bacteria to grow continuously over multiple generations while being dosed with antibiotics. Although theirs was not the first morbidostat device, the team designed a new, more effective version of the system for their experiments.
“It’s like an evolution machine, letting us watch the development of antibiotic resistance in real time and in an environment that more accurately models what happens to bacteria in a clinical setting than other approaches,” says Osterman. “This gives us a clearer and more comprehensive view of resistance than we’ve ever had before.”
Different bacteria develop resistance differently
By observing the bacteria’s evolution in the morbidostat and sequencing their genomes as they evolved, the researchers found that all three species had a similar pattern of resistance development. However, they also found subtle differences in the ways certain genes were expressed, particularly those that help bacteria remove toxins, a critical process in developing resistance.
“It’s like three remakes of the same movie by three different directors, and their comparison gives us a wealth of information to guide the development and use of antibiotics,” says Osterman.
Understanding resistance is critical to reducing its harm
Working with Roche, the team has completed similar studies on several other classes of antibiotic drugs, which is helping Roche identify promising candidates for antibiotics that are less prone to resistance.
And because antibiotic resistance is often not assessed in drug candidates until years into the process, using resistance to screen for drug candidates this way could save the biomedical industry millions of dollars and help patients benefit from effective drugs sooner.
“A completely ‘irresistible’ drug is a holy grail, something we can never truly achieve,” says Osterman. “But some drugs are less resistible than others, and our methods allow us to figure out which is which in a systematic way.”
In addition to helping develop new drugs, the researchers claim that their findings are easily translatable to the clinic, where doctors can use detailed knowledge of resistance to select optimal drug combinations with less likelihood of failure due to resistance.
“We are moving away from trial-and-error approaches in medicine and moving toward being able to predict exactly what drugs will work best for each patient,” says Osterman. “It is going to take time, effort and money to make this happen, but it will all be worth it if we’re able to alleviate the threat of antibiotic resistance and help save lives, which I’m confident can be done.”
Institute News
Laura Martin-Sancho rises to the challenge of COVID-19
The journal Molecular Cell recently asked Laura Martin-Sancho to share her experience working on SARS-CoV-2 during the pandemic
COVID-19 altered our lives and pushed scientific research to operate at breakneck speed, leading to significant breakthroughs in record time. The journal Molecular Cell recently asked experts in the field—including Laura Martin-Sancho—about the challenges they faced in transitioning, rapidly but safely, to working on the virus while navigating the shutdown. Their voices converge on the importance of teamwork, forging new collaborations, and working toward a shared goal.
Here is what Laura had to say:
I remember learning about viral pandemics in university and thinking about the challenges of working with novel viruses. Of course, we virologists contemplate the idea of a global viral pandemic and we discuss this at length in grants and in research articles, but how do you respond when confronted by it? It all started in February 2020 as I was completing my postdoc studying respiratory viruses. The lab had been closely following the worrying news coming from China and decided to drop everything else and work full time on SARS-CoV-2. Once we received the virus in March, it was a race against the clock to get the right conditions, the right cells, and the right reagents to propagate the virus to high enough amounts to start testing small compounds for antiviral activity. With a starting material of barely 100 μl received from BEI Resources, and long lonely hours in the BSL3, I felt a massive relief when I finally saw that the virus was replicating. Soon after, we had optimized experimental conditions and high enough viral yields to begin the essential experiments.
It was a remarkable feeling to have the whole research institute to just the seven of us. It was just me and three other lab members, our PI, Sumit Chanda, and two members of the institute safety department. With nobody around, it felt like we were apocalyptic survivors racing to find a cure. With a non-stop schedule from 8 am to 10 pm in the lab and trying to play catch up with an everyday-evolving literature, we were barely getting any sleep but never felt so energized. I felt so supported and inspired by my family and friends back home in Spain, which was one of the initial pandemic epicenters in Europe. I felt it was our responsibility to keep going and to make discoveries that could have a meaningful contribution. And so we did. In only a few months, we evaluated thousands of small compounds (initially in collaboration with Hong Kong University, then in house), we identified the innate immune sensor for SARS-CoV-2, and we illuminated the cellular antiviral landscape to SARS-CoV-2. Of course, this wouldn’t have been possible without the expertise and assistance from our countless collaborators across the globe. Indeed, a story to tell my grandkids.
Drug candidate blocks autophagy, a cellular recycling process that cancer cells hijack as a way to resist treatment
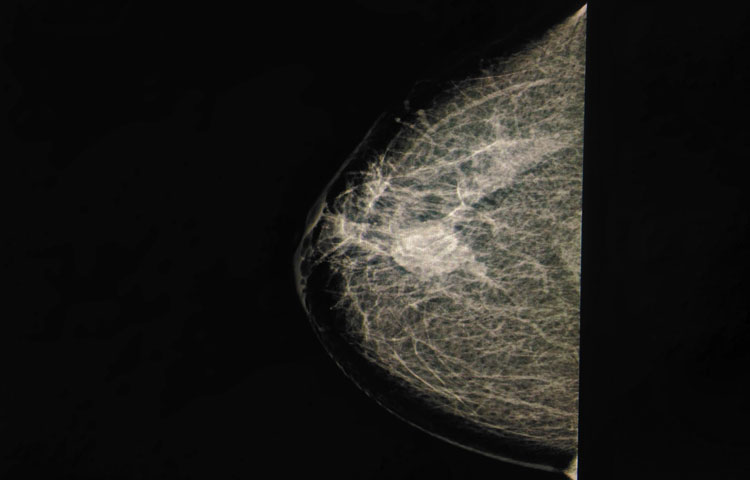
Scientists at Sanford Burnham Prebys Medical Discovery Institute have designed a next-generation drug, called SBP-7455, which holds promise as a treatment for triple-negative breast cancer—an aggressive cancer with limited treatment options. The drug blocks a cellular recycling process called autophagy, which cancer cells hijack as a way to resist treatment. The proof-of-concept study was published in the Journal of Medicinal Chemistry.
“Scientists are now learning that autophagy is one of the main ways that cancer cells are able to survive, even in the presence of growth-blocking treatments,” says Huiyu Ren, a graduate student in the laboratory of Nicholas Cosford, PhD, at Sanford Burnham Prebys, and first author of the study. “If all goes well, we hope this compound will stop cancer cells from turning on autophagy and allow people with triple-negative breast cancer to benefit from their treatment for as long as possible.”
Cells normally use autophagy as a way to recycle waste products. However, when cancer cells’ survival is threatened by a growth-blocking treatment, this process is often “revved up” so the cancer cell can continue to receive nutrients and keep growing. Certain cancers are more likely to rely on the autophagy process for survival, including breast, pancreatic, prostate and lung cancers.
“While this study focused on triple-negative breast cancer, an area of great unmet need, we are actively testing this drug’s potential against more cancer types,” says Cosford, professor and deputy director in the National Cancer Institute (NCI)-designated Cancer Center at Sanford Burnham Prebys and senior author of the study. “An autophagy-inhibiting drug that stops treatment resistance from taking hold would be a great addition to an oncologist’s toolbox.”
About 15% to 20% of all breast cancers are triple negative, which means they do not respond to hormonal therapy or targeted treatments. The cancer is currently treated with surgery, chemotherapy and radiation, and is deadlier than other breast cancer types. If the tumor returns, other treatments such as PARP inhibitors or immunotherapy are considered. People under the age of 50 are more likely to have triple-negative breast cancer, as well as women who are Black, Hispanic, and/or have an inherited BRCA mutation.
An optimized drug
In this study, the scientists optimized a first-generation drug they created in 2015. The result is a compound called SBP-7455 that blocks two autophagy proteins, ULK1 and ULK2. SBP-7455 exhibits promising bioavailability in mice and reduces autophagy levels in triple-negative breast cancer cells, resulting in cell death. Importantly, combining the drug with PARP inhibitors, which are currently used to treat people with recurrent triple-negative breast cancer, makes the drug even more effective.
“We are hopeful that we have found a new potential therapy for people living with triple-negative breast cancer,” says Reuben Shaw, PhD, a study author and professor in the Molecular and Cell Biology Laboratory and director of the NCI-designated Cancer Center at the Salk Institute. “We envision this drug being used in combination with targeted therapies, such as PARP inhibitors, to prevent cancer cells from becoming treatment resistant.”
Next, the scientists plan to test the drug in mouse models of triple-negative breast cancer to confirm that the compound can stop tumor growth in an animal model. In parallel, they will continue optimization efforts to ensure the drug has the greatest chance of clinical success.
“Triple-negative breast cancer is one of the hardest cancers to treat today,” says Ren. “I hope that our research marks the start of a path to successful treatment that helps more people survive this aggressive cancer.”
Additional study authors include Nicole A. Bakas, Mitchell Vamos, Allison S. Limpert, Carina D. Wimer, Lester J. Lambert, Lutz Tautz, Maria Celeridad and Douglas J. Sheffler of Sanford Burnham Prebys; Apirat Chaikuad and Stefan Knapp of the Buchmann Institute for Molecular Life Sciences and Goethe-University Frankfurt; and Sonja N. Brun of the Salk Institute.
This work was supported by the National Institutes of Health (P30CA030199, T32CA211036), Epstein Family Foundation, Larry L. Hillblom Foundation (2019-A-005-NET), Pancreatic Cancer Action Network (19-65-COSF), SGC—a registered charity that receives funds from AbbVie, Bayer Pharma AG, Boehringer Ingelheim, Canada Foundation for Innovation, Eshelman Institute for Innovation, Genome Canada through Ontario Genomics Institute [OGI-196], EU/EFPIA/OICR/McGill/KTH/Diamond, Innovative Medicines Initiative 2 Joint Undertaking (875510), Janssen, Merck KGaA, Merck & Co, Pfizer, São Paulo Research Foundation-FAPESP, Takeda, and Wellcome.
The study’s DOI is 0.1021/acs.jmedchem.0c00873.
Institute News
Mining “junk DNA” reveals a new way to kill cancer cells
Scientists unearth a previously unknown vulnerability for cancer and a promising drug candidate that leverages the approach
Scientists at Sanford Burnham Prebys have uncovered a drug candidate, called F5446, that exposes ancient viruses buried in “junk DNA” to selectively kill cancer cells. Published in the journal Cell, the proof-of-concept study reveals a previously unknown Achilles’ heel for cancer that could lead to treatments for deadly breast, brain, colon and lung cancers.
“We found within ‘junk DNA’ a mechanism to stimulate an immune response to cancer cells, while also causing tumor-specific DNA damage and cell death,” says Charles Spruck, PhD, assistant professor in the National Cancer Institute (NCI)-designated Cancer Center and senior author of the study. “This is a very new field of research, with only a handful of papers published, but this has the potential to be a game-changer in terms of how we treat cancer.”
Since the human genome was fully sequenced in 2003, scientists have learned that our DNA is filled with some very strange stuff—including mysterious, noncoding regions dubbed “junk DNA.” These regions are silenced for a reason—they contain the genomes of ancient viruses and other destabilizing elements. An emerging area of cancer research called “viral mimicry” aims to activate these noncoding regions and expose the ancient viruses to make it appear that a cancer cell is infected. The hypothesis is that the immune system will then be triggered to destroy the tumor.
A one-two punch to cancer
In the study, Spruck and his team set out to find the molecular machinery that silences “junk DNA” in cancer cells. Using sophisticated molecular biology techniques, they found that a protein called FBXO44 is key to this process. Blocking this protein caused the noncoding sections of DNA to unwind—but not for long.
“When we revealed noncoding regions, which aren’t meant to be expressed, this caused DNA breakage. This told the cell that something is deeply wrong, and it committed suicide,” explains Spruck. “At the same time, the DNA of the ancient virus was exposed, so the immune system was recruited to the area and caused more cell death. So, we really delivered a one-two punch to cancer.”
The scientists then showed that a drug that targets the FBXO44 pathway, called F5446, shrank tumors in mice with breast cancer. The drug also improved the survival of mice with breast cancer that were resistant to anti-PD-1 treatment, an immunotherapy that is highly effective but often stops working over time. Additional studies in cells grown in a lab dish showed that the drug stops the growth of other tumors, including brain, colon and lung cancers.
The scientists also conducted many experiments to show that this silencing mechanism only occurs in cancer cells, not regular cells. Analysis of patient tumor databases confirmed that FBXO44 is overproduced in many cancers and correlated with worse outcomes—further indicating that a drug that inhibits this protein would be beneficial.
Moving the research toward people
As a next step, the scientists are working with the Conrad Prebys Center for Chemical Genomics to design an FBXO44 pathway-inhibiting drug that is more potent and selective than F5446. This state-of-the-art drug discovery facility is located at Sanford Burnham Prebys.
“Now that we have a compound that works, medicinal chemists can make modifications to the drug so we have a greater chance of success when we test it in people,” says Jia Zack Shen, PhD, staff scientist at Sanford Burnham Prebys and co-first author of the study. “Our greatest hope is that this approach will be a safe and effective pan-cancer drug, which maybe one day could even replace toxic chemotherapy.”
Institute News
COVID-19 vaccines: Our experts weigh in on the historic news
There are now two experimental vaccines for COVID-19 that are more than 90% effective—a remarkable development that has made the world collectively exhale. We caught up with our leading COVID-19 researchers to get their take on the update—including whether we are “out of the woods” and where they were when they heard the news.
Sumit Chanda, PhD, virologist I was at work, obsessively refreshing my browser to follow the election results when the first press release about the Pfizer vaccine popped up. When I heard 90% efficacy, I was super excited. I had sort of a sigh of relief. Then I read the fine print, and I started to have more guarded optimism. I’m not popping the champagne yet. But I’m putting it on ice.
The 90% measurement was taken starting only one week after the second booster shot. That’s not a lot of time, and with a pretty small number of people. What I am really looking for is how many people are protected two months and six months after the booster shot. That’s when I’m going to get really excited. We know that 90% is the ceiling, now we need to know where the floor is. Even if efficacy drops from 90 to 70%, that is still really great.
This is also why we will likely need multiple vaccines, and with different mechanisms of protection. This vaccine also has to be kept at -70 degrees Celsius, which presents a logistical challenge to say the least. Most doctor’s offices don’t have this type of specialized equipment, not to mention rural areas or less developed countries.
Today’s news that the Moderna vaccine is at least as effective as Pfizer’s is equally great news. However, we are still going to need antivirals. Between people who may not respond to these vaccines, can’t get the vaccines, or simply don’t want to take them, there is still going to be a lot of people who catch COVID-19. Luckily there are some antiviral options that are looking really good, including an antibody from Lilly that just got Emergency Use Authorization from the FDA.
With all this said, this is unequivocally good news. I am optimistic that we will have several vaccines that are usable in the next couple months. But for now, we need to mask up and keep social distancing.
Step inside Sumit Chanda’s lab where he and his colleagues are racing to find a potential treatment for COVID-19.
Carl Ware, PhD, immunologist and clinical trial participant
I first heard the news about the Pfizer vaccine on the radio when I was listening to KPBS’ surf report (Scott Bass is a poet). As an immunologist studying coronaviruses and a volunteer in the Moderna vaccine trial, I’m following all of the results closely. I immediately turned the volume up.
NBC San Diego spoke with Dr. Carl Ware about his experience participating in a clinical trial testing Moderna’s vaccine for COVID-19.
The news is very encouraging, and certainly shines a brighter light at the end of the proverbial tunnel. 90% effectiveness is very impressive. My excitement is mostly based upon earlier trial results showing that the vaccines are safe and effective in stimulating the immune system. However, those trials only involved several hundred people in comparison to the tens of thousands of volunteers in the latest results, so these developments are very encouraging. It gives us a much better understanding of how the vaccine may work in the general population.
However, questions will need to be answered about the efficacy in people over the age of 65 and other susceptible populations, the longevity of immunity, and long-term safety. Fortunately, these results will be scrutinized by scientists that are the best in the world. I have full confidence in their analysis.
The effort to make a vaccine so quickly is truly an outstanding accomplishment. It’s not a race to be first, but first to stop the virus. This war against an unseen enemy will require multiple strategies to truly end this pandemic. Right now I am keeping an eye out for data that shows the long-term protection of these vaccines, and looking forward to results from my colleague Sumit Chanda, who has been racing to find existing drugs that could treat people who do become sick with COVID-19.
I learned about the Pfizer-BioNTech vaccine news last Monday morning. I had just woken up and was enjoying a cup of coffee when I read the press release. Here, they reported the results to date of their vaccine clinical trial showing 90% protection from COVID-19 infection. I felt very happy and very hopeful. Being from Spain, one of the countries that has been most affected by COVID-19, and having all my family over there, I felt this was the news we all have been waiting for a long time.
While this 90% might not hold by the end of the trial as more cases are reported, it still brings a lot of hope. Especially since many vaccines currently under clinical trials, including Moderna’s, use a similar approach. So we have even more reasons to be optimistic.
Future challenges for these vaccines will be to determine if they can prevent transmission from asymptomatic people with COVID-19. As clinical trial participants were not tested for COVID-19 throughout the study, and only symptomatic cases were reported, the question remains as to whether vaccinated people can still transmit the disease.
We also still don’t know how long the protection elicited by the vaccine lasts, which will determine whether and how frequently we will need a vaccine boost. In addition, more data are needed to evaluate if these vaccines can protect against severe COVID-19 or whether different age groups or ethnicities are protected. Only time will tell.
Meet the scientists on the front lines with coronavirus, including Dr. Martin-Sancho.
Institute News
A scientist’s perspective on the coronavirus (COVID-19) pandemic
Infectious disease expert Sumit Chanda tells us how his team is combating the virus, and the advice he gives his loved ones.
Since the first case of coronavirus (COVID-19) was identified in December 2019, the respiratory virus has swept across the globe. Cases have been confirmed on every continent but Antarctica, prompting the World Health Organization to declare COVID-19 an official pandemic.
As the world grapples with the ongoing outbreak, we spoke with Sumit Chanda, PhD, an infectious disease expert and director of Sanford Burnham Prebys’ Immunity and Pathogenesis Program, to get his perspective on the pandemic and learn what Sanford Burnham Prebys scientists are doing to find effective treatments for COVID-19.
What is coronavirus? Coronaviruses are a large family of viruses common in animals, but they can leap to humans, causing illnesses ranging from a common cold to severe respiratory diseases such as pneumonia, Middle East respiratory syndrome (MERS), and severe acute respiratory syndrome (SARS).
Were you surprised by the virus’s rapid spread? Why or why not? Once there was evidence of person-to-person transmission outside of China, the rapid global spread of the virus was not surprising. Since this is a new virus, there is no natural immunity in the human population to slow the spread of the pathogen. Furthermore, respiratory viruses are among the most easily spread microbes and thus considered to have high pandemic potential.
Is there a vaccine for COVID-19? Since this is a new coronavirus, there is no vaccine—and developing one can take several years.
How are Sanford Burnham Prebys scientists working to combat COVID-19? As we speak, our scientists are looking to find known drugs that can inhibit the virus. Typically, it can take five to 10 years to bring a new drug to the market. However, the approach we are taking at Sanford Burnham Prebys, known as drug repositioning, can cut this development time dramatically. Since we are looking at FDA-approved drugs that are proven to be safe in humans, these medicines could rapidly get to people infected with the virus. If successful, drug repositioning will likely be the fastest path to find a therapeutic solution for the virus.
Longer term, work has been ongoing to develop broad-spectrum antivirals. These medicines would work against many viruses, not just one. For example, if we had developed a broad-spectrum antiviral that works on MERS or SARS, it is likely it could be used for the current COVID-19 outbreak. Ideally, the therapy could be given prophylactically to block the rapid spread of the disease.
What are the benefits of drug repositioning? Drug repositioning is advantageous because FDA-approved drugs have already completed safety testing—meaning they have been used in people and are known to be safe. Safety testing can take years to complete. This means that if we do find a therapy that is effective against COVID-19, we can bring it to patients much faster than a novel treatment.
Any predictions for how far the virus will spread in the U.S.? We eagerly await large-scale testing for the virus so we can get a better understanding of how widespread it currently is in the U.S. It is difficult to predict a potential trajectory of viral spread in the U.S. until those numbers become available.
But as of now, I have not seen any evidence of disease containment. It will be instructive to see how the situation plays out in other advanced democracies that are coping with a viral outbreak, including South Korea and Europe, to get a better idea of what might happen here.
Get an inside look at the race to find a treatment for COVID-19.
What advice are you giving your loved ones? The advice I give my friends and family is to hope for the best, prepare for the worst. We are in uncharted waters.
Institute News
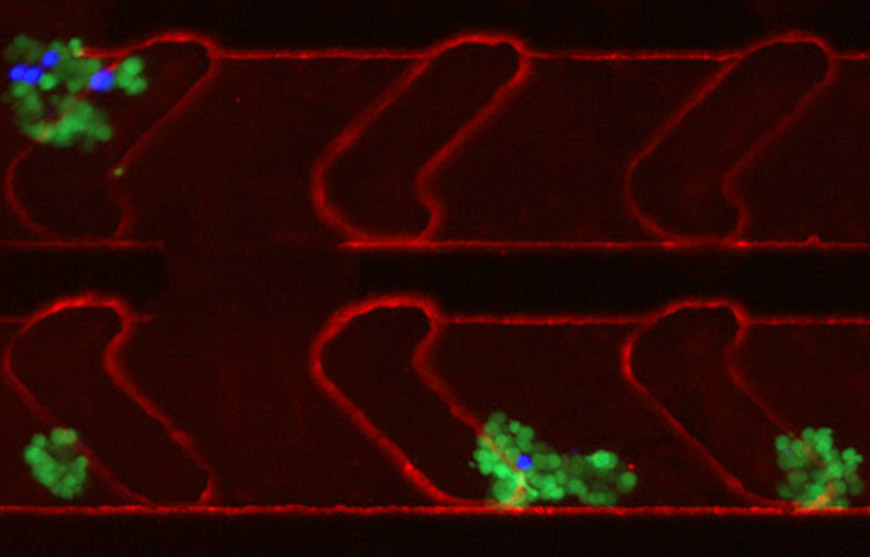
Capturing circulating cancer cell clusters using a new microfluidic device
Nearly 90 percent of cancer deaths are a result of metastases, when tumors spread to other vital organs. Researchers are learning that cancer metastases are not due to individual cells but rather distinct clusters of cancer cells that circulate and metastasize to other organs. However, obtaining these clusters to learn more about the metastatic process has proved difficult.
Now, in a study published in AIP Advances, researchers from Sanford Burnham Prebys, San Diego State University and TumorGen MDx™ have described a new microfluidic device that captures circulating cancer cell clusters.
“The reason for such little research activity on cancer clusters is the overwhelming difficulty of capturing these extremely rare samples from a patient’s blood sample,” says Peter Teriete, PhD, a study author and a research assistant professor at Sanford Burnham Prebys. “But we realized that if we’re ever going to understand the complex process of cancer metastasis, we’d need to develop a tool to easily find these clusters.”
To do so, the researchers first identified the basic requirements essential to collecting useful information from isolated cancer cell clusters. It involves a sample size large enough to likely contain appreciable numbers of cancer cell clusters (about 10 milliliters of whole blood), as well as using whole blood to preserve rare circulating clusters. Whole blood, however, requires special channel-coating procedures that reduce nonspecific binding properties to prevent biofouling. And the device channel dimensions must be of a suitable size to accommodate single cells and cancer cell clusters of varying diameters.
“Our device’s channel design had to generate microfluidic flow characteristics suitable to facilitate cell capture via antibodies within the coated channels,” Teriete explains. “So we introduced microfeatures—herringbone recesses—to produce the desired functionality. We also developed a unique alginate hydrogel coating that can be readily decorated with antibodies or other biomolecules. By connecting bioengineering with materials science and basic cancer biology, we were able to develop a device and prove that it performs as desired.”
The group’s microfluidic device brings a new therapeutic strategy to the fight against cancer metastasis. Capturing viable circulating cancer stem cell clusters directly from cancer patients is a novel approach for the development of new anti-metastatic drug therapies.
“Drug development that specifically targets distant metastases has been greatly restricted due to the lack of adequate tools that can readily access the metastatic cells responsible for cancer’s dissemination,” says Teriete. “Our microfluidic device will provide cancer researchers with actual human cancer cell clusters so they can begin to understand the critical mechanisms involved with metastasis and develop highly effective drugs that ultimately can save more cancer patients’ lives.”
Story materials courtesy of the American Institute of Physics. Content has been edited for style and length.